SITUATION:
This QuickHit was developed in response to questions from family caregivers and home care nurses inquiring about how to minimize the risk of blockages in central venous access devices (CVAD).
BACKGROUND:
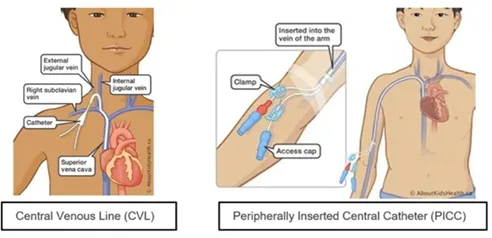
Many children with medical complexity rely on CVADs in home and community care for long-term intravenous therapy including medication administration, parenteral nutrition, dialysis, hydration, and blood sampling. Types of CVADs include central venous lines (CVL), peripherally inserted central catheters (PICC), and Ports.
?")
One potential complication associated with CVADs is catheter blockage. Blockages may result from thrombus formation within, surrounding, or at the tip of the catheter. Such obstructions can delay the timely administration of treatments or medications, posing significant safety risks to patients and families, particularly if hospital readmission is required to have the line unblocked or replaced. Furthermore, there is a risk that a thrombus may become dislodged and embolize to the lungs, causing a pulmonary embolism, which can lead to serious clinical complications.
ASSESSMENT:
There are different types and causes of CVAD blockages, which can affect how well the device functions. These blockages are categorized by their degree and type.
Degrees of Occlusion
- Complete occlusion: no ability to flush or withdraw blood from the CVAD.
- Partial occlusion: difficulty flushing and withdrawing blood, with noticeable resistance.
- Withdrawal occlusion: flushing is possible, but blood cannot be withdrawn.
Types of Occlusions
- Mechanical occlusions involve the infusion system.
- External causes include kinked or clamped tubing/CVAD, blocked filers or needleless connectors, or physical damage to the CVAD.
- Internal causes include internal kinks, improper tip placement, or tip migration.
- Chemical occlusions result from the mixing of incompatible medications or solutions, or from lipid buildup within the CVAD lumen.
- Thrombotic occlusions are caused by fibrin buildup or blood clots within the catheter or blood vessel.
A patent CVAD flushes without resistance and allows for blood return. Patency should be assessed daily by flushing each lumen and aspirating for blood return as per orders. Routine flushing and heparin locking helps ensure continued patency and reduces risk of thrombotic occlusions. The recommended frequency varies based on CVAD use:
- Continuous infusion: flush each lumen once daily.
- Intermittent use: flush before and after each use (e.g., medication or blood sampling), followed by a heparin lock.
- Not in use: flush and heparin lock at least once within a 24-hour period.
Prescribed heparin doses are sub-therapeutic and calculated based on child’s weight.
RECOMMENDATION:
Connected Care recommends the following to maintain patency and minimize the risk of CVAD blockages in home and community:
- Confirm the child’s care plan on maintaining patency of the CVAD including flushing and heparin locking.
- Flush using a turbulent technique (push-pause method) with normal saline to effectively clear the lumen and reduce the risk of occlusion.
- Ensure the CVAD is flushed and heparin locked with the prescribed dose at least once daily when it is not in use or infusing. If CVAD is continuously infusing, ensure that it is flushed once daily.
- Assess for signs of partial or complete blockage, such as resistance when flushing or inability to withdraw blood. If you identify resistance or potential blockage, address it promptly to avoid missed medications or delayed treatments by:
- Tracing the line from the medication source and infusion pump to the patient to check for any external mechanical blockages (e.g., kinked tubing, closed clamps).
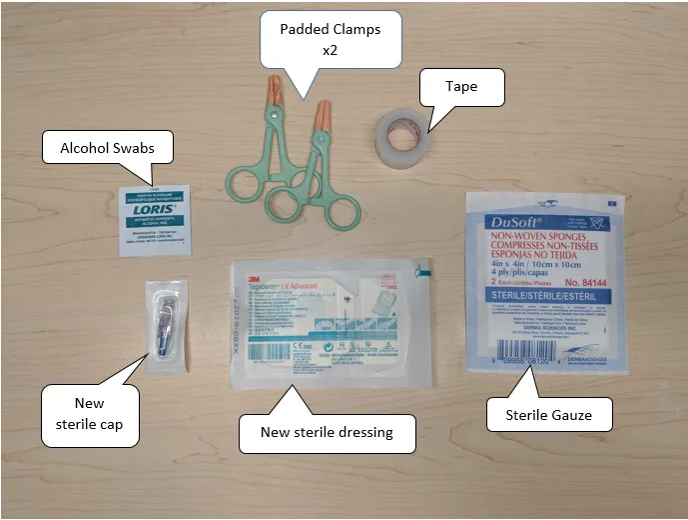
- Performing a cap change, if possible.
- Flushing the CVAD using the turbulent push-pause technique.
- Repositioning the child while flushing (e.g., raising the arm or changing head of position).
- If unsuccessful, promptly contact the child’s care team. For administration of timed or critical IV medications, advise the family to bring the child to the emergency department for IV medication administration and occlusion treatment.
- See the image below for heparin locking guidelines.
- For patients with CVADs weighing less than 10kg or those receiving anticoagulation therapy (e.g., heparin or warfarin), sub-therapeutic doses of heparin should be maintained by limited heparin locking to no more than three times per day.
- For haemodialysis or apheresis patients:
- If high-concentration heparin (greater than 100 units/mL) is used, the heparin MUST be withdrawn to the lumen volume before proceeding.
- Do not flush heparin or sodium citrate 4% into the patient.
- Withdraw all heparin or sodium citrate 4% from each catheter lumen prior to any use, including dialysis, aphresis, re-heparinization, or flushing
?")
For additional information on how to heparin lock a central venous access device, click here to visit AboutKidsHealth, or consider a Connected Care Live consult