SITUATION:
This QuickHit was informed by a Connected Care Live consult regarding a child’s dislodged gastrostomy tube.
BACKGROUND:
Many children with medical complexity rely on feeding tubes to support nutrition, hydration and/or medication administration. There are different types of feeding tubes, placed in specific part(s) of the gastrointestinal system. Examples of these tubes include:
- Gastrostomy (G) Tubes: provide access to stomach
- Gastrojejunostomy (GJ) Tubes: provide access to intestine
- Combination Gastrostomy/Gastrojejunostomy (G/GJ) Tubes: provide access to stomach and intestine
- Jejunal (J) Tubes: provide access to intestine
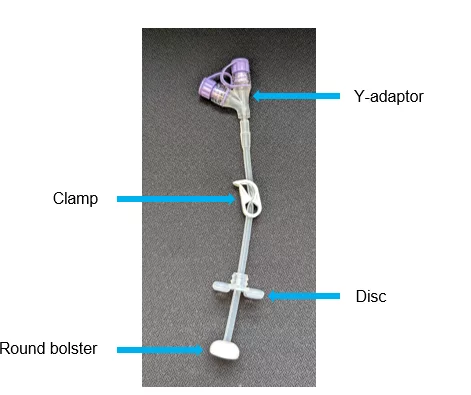
These feeding tubes are inserted in a hospital by a specially trained doctor. During the insertion procedure, a small opening (called a stoma) is made in the child’s abdomen or belly wall. A tunnel (called a tract) is created from the skin into the child’s stomach or intestine. The feeding tube is placed into this tract. Below is an image of a gastrostomy tube stoma, which shows what the opening looks like once the tube is in place.

ASSESSMENT:
If a feeding tube accidentally comes out – also known as becoming dislodged – it is important to act quickly to prevent the tract from closing. If nothing remains in the tract, it will begin to narrow and close. To prevent this from happening, a Foley catheter needs to be inserted into the stoma and tract as shown below.

An emergency dislodgement kit containing the following components should always be with the child in case a dislodgment happens:

- A Foley catheter – The same French size as child’s feeding tube and one size smaller
- Water-based lubricating jelly – to lubricate the tip of the Foley catheter before insertion
- Tape – to secure the Foley catheter to the child’s abdomen after insertion
- pH strips and colour reference guide – to confirm that the Foley catheter is in the stomach by checking the pH of the stomach contents
- 1 ENFit syringe – to check the pH
- Water – to inflate the Foley catheter balloon
- 1 Slip-Tip Syringe – to fill the Foley catheter balloon
- An adaptor and extension set – to close the Foley catheter, and to access the Foley catheter as a temporary
The decision whether to insert a Foley catheter and inflate the balloon on a Foley catheter depends on several factors. Exceptions are detailed in the recommendation section below. It is important to know the following details when responding to feeding tube dislodgement:
- What type of tube does the child have?
- G, GJ, Combo G/GJ, J -tube
- How was it put in?
- Interventional Radiologist or Surgery
- What is the French size of the dislodged feeding tube?
- e.g. 12Fr, 14Fr, 16FR
- How long ago was the first feeding tube put in?
- Less than 8 weeks ago
- Greater than 8 weeks ago
RECOMMENDATION:
Connected Care recommends the following most up to date practice related to managing dislodged feeding tubes:
- Always confirm the child has their emergency dislodgement kit with them and that it is fully stocked. If they do not have a kit, gather the appropriate supplies into a clean zip-lock bag. If the required supplies are needed but missing or unavailable, partner with family and contact the child’s G-tube specialist or bring them to the emergency department
- Verify the tube details as described in the assessment section.
- If the feeding tube that was dislodged was a balloon G tube and the balloon is not broken, wash the tube and re-insert it back into the stoma as shown in this video. If the child has a Primary MIC KEY balloon G-tube, refer to this article to learn what to do if it dislodges before and after 8 weeks since it’s insertion.
- If the balloon feeding tube cannot be re-inserted OR the dislodged tube is not a balloon G tube, follow the steps outlined below and in this video.
- Wash your hands and the skin around the child’s stoma with soap and water. Obtain the Foley catheter that is the same size as the child’s dislodged feeding tube. Lubricate the tip of the Foley catheter. Measure the Foley catheter against your index finger.
- If child weighs < 3 kg: Measure 3-4 cm (1/2 of your index finger)
- If child weighs > 3 kg: Measure 4-6 cm (full index finger)
- With your dominant hand, insert the lubricated Foley catheter into the stoma and tract at the length you measured to. Tape the Foley catheter to the child’s abdomen. If you cannot insert the same size (e.g. 14Fr), use a Foley catheter one French size smaller (e.g. 12Fr).
- Based on the tube details, refer to the chart below to guide your next steps.
- Wash your hands and the skin around the child’s stoma with soap and water. Obtain the Foley catheter that is the same size as the child’s dislodged feeding tube. Lubricate the tip of the Foley catheter. Measure the Foley catheter against your index finger.

- Contact child’s G tube specialist or go to the nearest emergency department if you cannot insert the Foley catheter into the stoma or if you cannot verify the Foley catheter is in the stomach using pH strips.
- Stop using the Foley catheter to administer feeds/medications and seek medical attention if the child has a hard bloated stomach, severe pain in the stomach, bleeding, vomiting, coughing, gagging, sudden high fever, diarrhea, problems with feeds and liquids getting into the lungs or breathing problems. Partner with family and child’s G tube specialist to arrange to have the child’s original G, GJ or G/GJ tube replaced.
- If the child is now using a temporary Foley catheter as their feeding tube, partner with family and child’s G tube specialist to arrange to have the child’s original G, GJ or G/GJ tube replaced.
- Exceptions include:
- DO NOT insert a foley catheter into the stoma/tract if the child’s feeding tube was inserted by a surgeon less than 8 weeks ago OR if the child had gastrointestinal surgery in the last 8 weeks. In these cases, partner with the child’s family and bring them to the emergency department for further management.
- If a child’s surgically inserted J-tube dislodges after 8 weeks since it’s insertion, insert the Foley catheter into the stoma and secure it to the child’s abdomen with tape. Partner with family for next steps because placement in the intestine cannot be checked with pH strips. The surgeon who inserted the child’s J tube may have advised the family that the foley catheter position needs to be checked with x-ray in hospital before inflating the balloon or before using the tube.
To learn more about what to do if a feeding tube fully dislodges, visit the following AboutKidsHealth article: G/GJ tubes: What to do if your child’s feeding tube is pulled out.