SITUATION:
This QuickHit was informed by recent inquiries from home and community care providers seeking clarification on the differences between active and non-active hemodialysis/apheresis central venous access devices (CVADs) and best practices for care of these CVADs in home and community settings.
BACKGROUND:
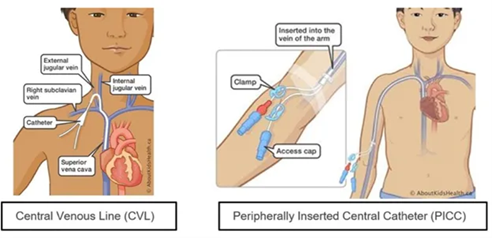
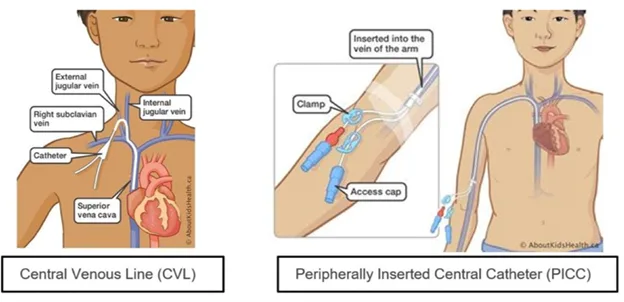
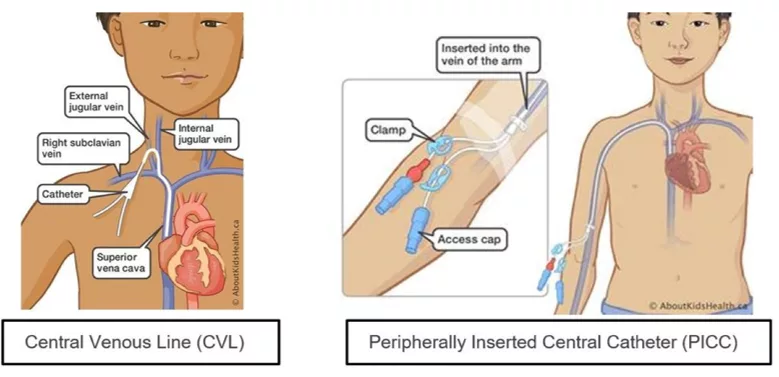
Children with medical complexity often rely on CVADs in home and community care settings for long term intravenous therapies, including medication administration, parenteral nutrition, dialysis, hydration, and blood sampling. Hemodialysis/apheresis CVADs are a specialized type of CVAD used when a child requires hemodialysis and/or apheresis. These devices differ from other CVADs because their larger catheter diameter allows for the high flow rates needed for rapid blood withdrawal and return.
?")
Hemodialysis/apheresis CVADs may be classified as active or non-active.
- An active hemodialysis/apheresis CVAD is one that is currently being used for dialysis and/or apheresis treatments.
- A non-active hemodialysis/apheresis CVAD is no longer required for dialysis and/or apheresis but remains in place for other clinical purposes, such as medication administration or hydration.
Children with active hemodialysis/apheresis CVADs may transition to non-active status once dialysis and/or apheresis is fully completed, such as following stem cell collection or kidney transplantation.
ASSESSMENT:
The child’s healthcare team determines whether a hemodialysis/apheresis CVAD is active or non-active based on the child’s current clinical needs. It is important to understand this classification because care requirements differ significantly between active and non-active devices, particularly related to maintaining catheter patency. The child’s healthcare team will clearly outline the required care in the medical orders.
The differences in maintaining patency for active and non-active hemodialysis/apheresis CVADs is outlined below:
| Active Hemodialysis/Apheresis CVAD | Non-Active Hemodialysis/Apheresis CVAD | |
| Flushing/Locking Frequency | Weekly and/or after intermittent use | Daily and/or after intermittent use |
| Locking Solution | High-dose heparin (1000 units/mL) or other locking solutions (i.e. KiteLock, Sodium Citrate 4%) | Low dose heparin (100 units/mL) or other locking solutions (i.e. KiteLock, Sodium Citrate 4%) |
RECOMMENDATION:
Connected Care recommends the following best practices when caring for children with active and non-active hemodialysis/apheresis CVADs in home and community:
- Confirm the type of CVAD, whether it is active or non-active, and review the current medical orders for maintaining patency before providing any care.
- If a child’s CVAD transitions from active to non-active while at home, obtain updated medical orders to reflect the new locking solution, dose, and frequency required to maintain patency.
- If an active hemodialysis/apheresis CVAD was locked with high-dose heparin (concentration of 1000 units per mL), KiteLock, or Sodium Citrate 4%, withdraw the locking solution prior to flushing or accessing the CVAD, as these solutions must not be flushed into the catheter.
- Follow medical orders carefully, as hemodialysis/apheresis CVADs vary in lumen size and volume, which directly affects the required locking solution volume and dose.
- Ensure a CVAD emergency kit remains with the child at all times.
For additional information, review AboutKidsHealth resources:
- Aseptic Non-Touch Technique
- Heparin Locking
- CVAD Dressing Change Procedure
- CVAD Cap Change Procedure